|
|
|
Management of Patients With Stable Ischemic Heart
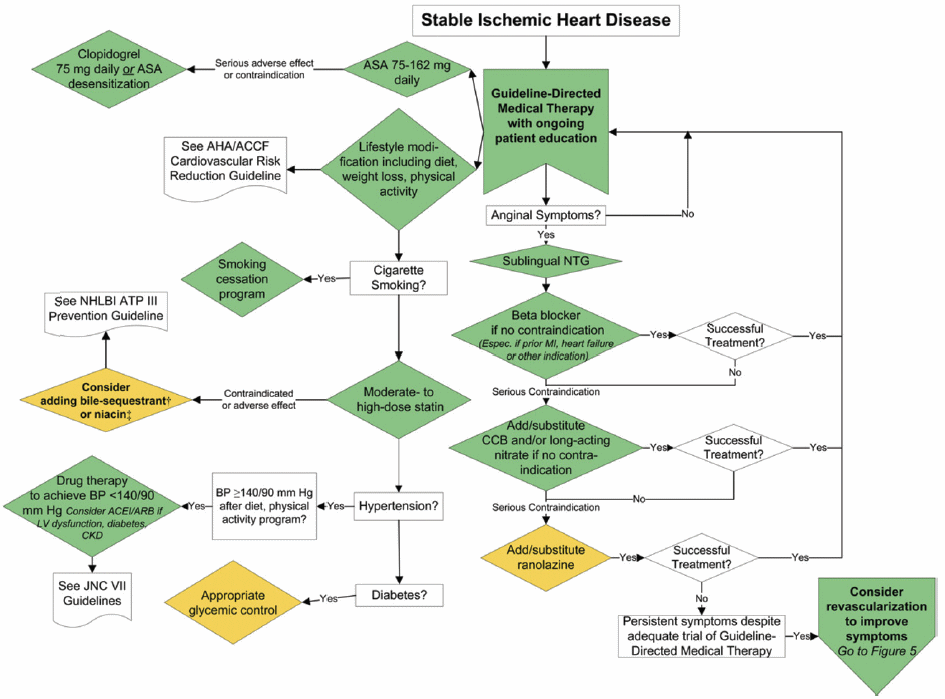
Disease: |
|
|
|
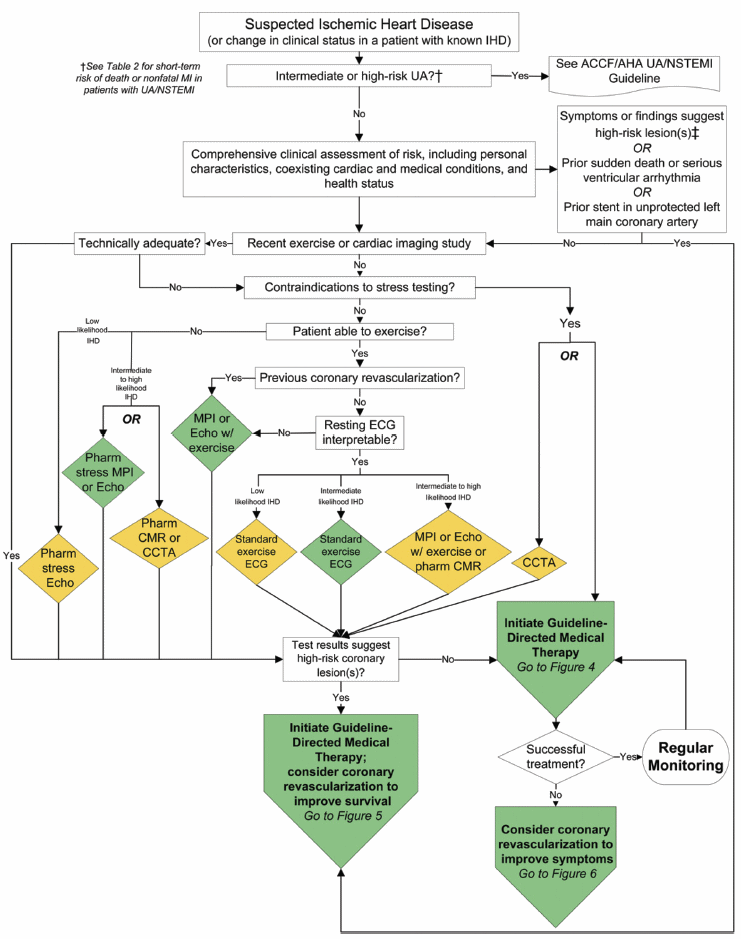
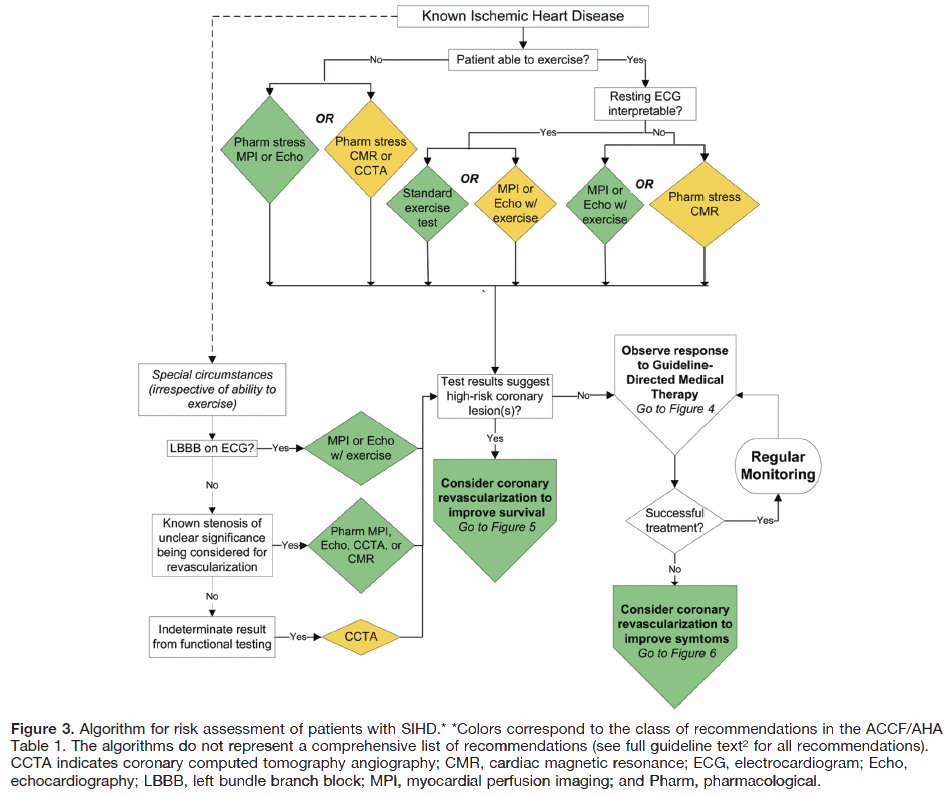
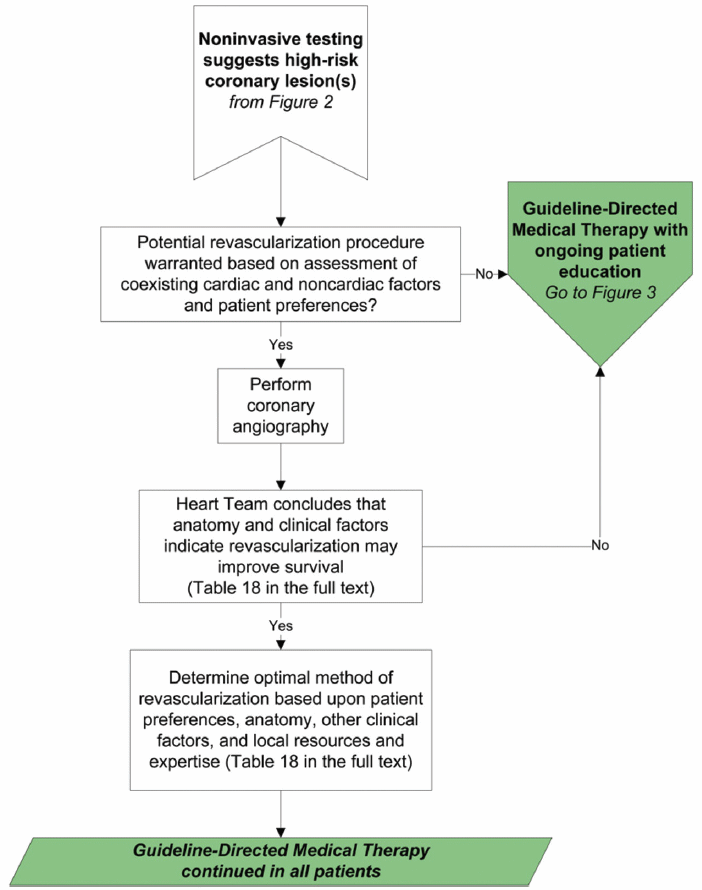
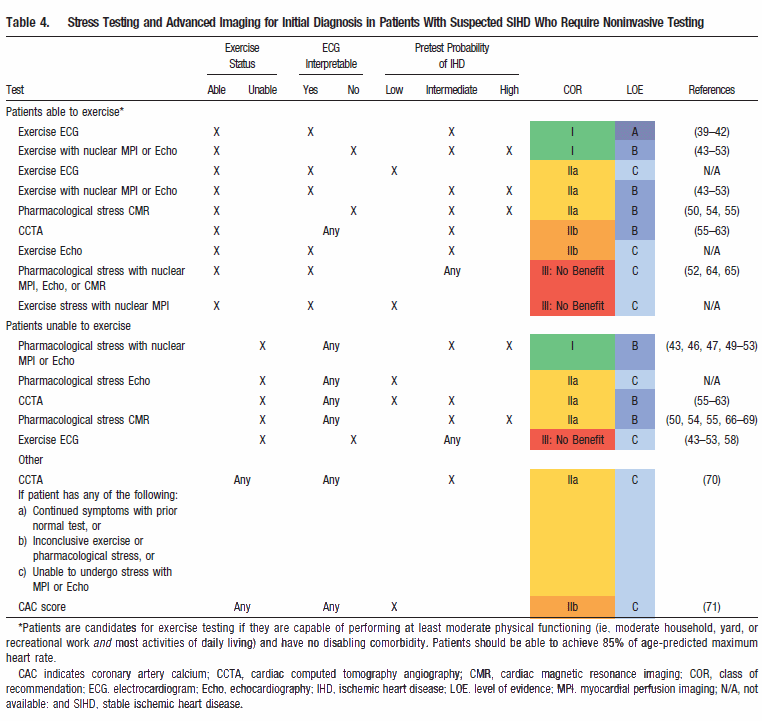
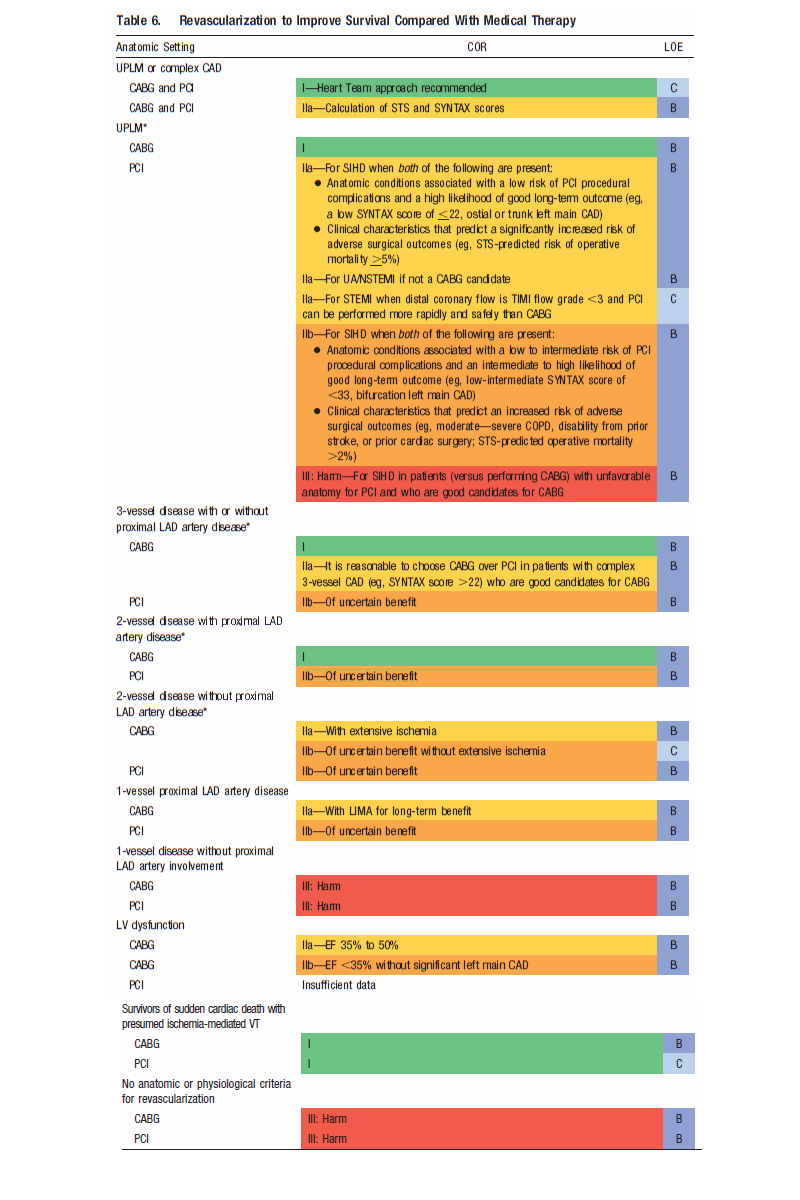
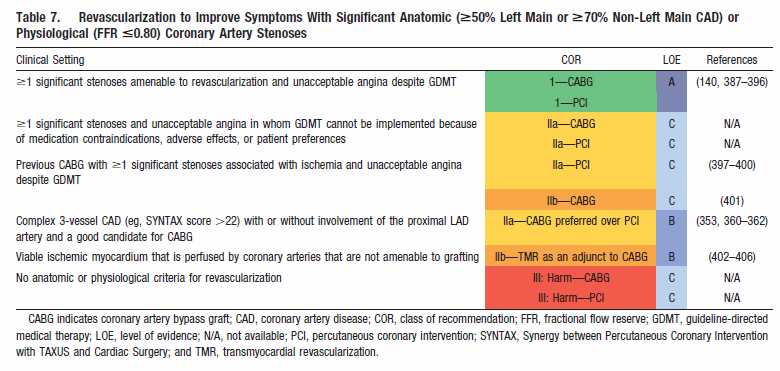
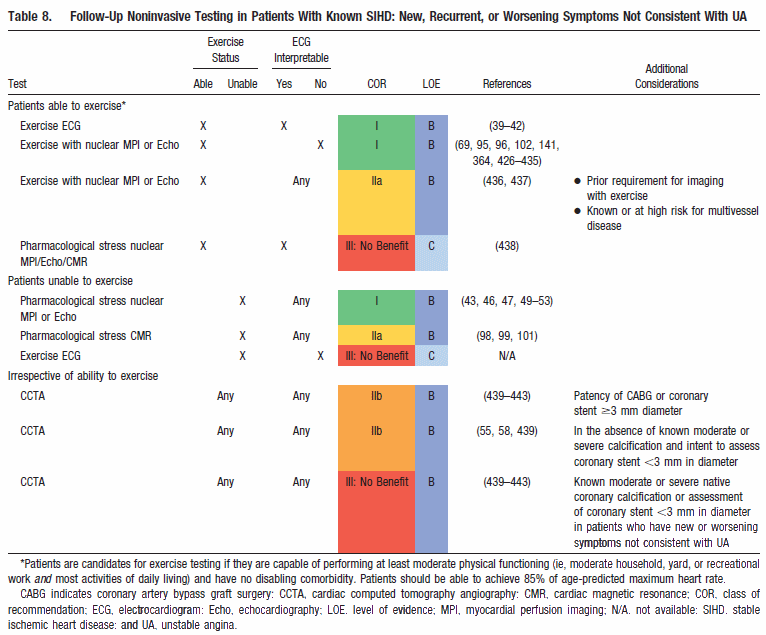
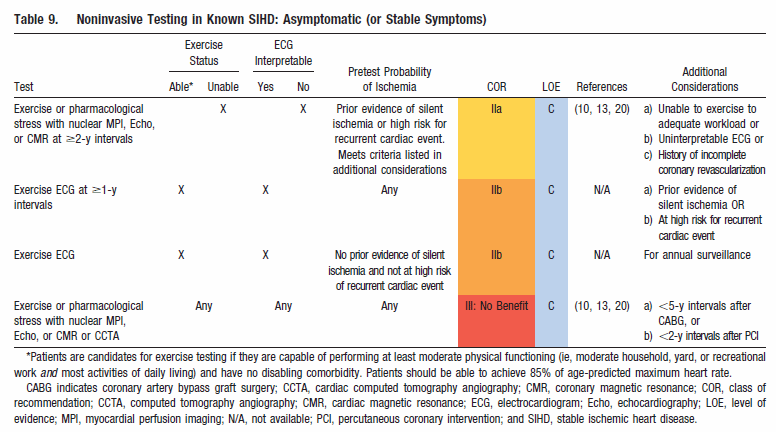
Perspective: The following are 10 points to remember from the November 2012 guidelines for the diagnosis and management of patients with stable ischemic heart disease (SIHD): 1. Choices about diagnostic and therapeutic options should be made through a process of shared decision making involving the patient and provider, with the provider explaining information about risks, benefits, and costs to the patient. 2. Coronary computed tomography angiography (CTA) is reasonable for patients with an intermediate pretest probability of IHD who: a) have continued symptoms with prior normal test findings, or b) have inconclusive results from exercise or pharmacological stress testing, or c) are unable to undergo stress testing with nuclear myocardial perfusion imaging (MPI) or echocardiography. 3. A normal exercise nuclear MPI study or a normal exercise stress echocardiogram during which the age-predicted target heart rate is achieved is associated with a very low annual risk of cardiac death and acute myocardial infarction (MI) (generally <1%) in both men and women. 4. Lifestyle modifications, including daily physical activity and weight management, are strongly recommended for all patients with SIHD. For all patients, the clinician should encourage 30-60 minutes of moderate-intensity aerobic activity, such as brisk walking, at least 5 days and preferably 7 days per week. 5. Treatment with aspirin 75-162 mg daily should be continued indefinitely in the absence of contraindications in patients with SIHD. 6. Beta-blocker therapy should be started and continued for 3 years in all patients with normal left ventricular function after MI or acute coronary syndrome. Angiotensin-converting enzyme inhibitors should be prescribed in all patients with SIHD who also have hypertension, diabetes mellitus, left ventricular ejection fraction of 40% or less, or chronic kidney disease, unless contraindicated. 7. Ranolazine can be useful when prescribed as a substitute for beta-blockers for relief of symptoms in patients with SIHD if initial treatment with beta-blockers leads to unacceptable side effects or is ineffective, or if initial treatment with beta-blockers is contraindicated. 8. Coronary artery bypass grafting (CABG) surgery is probably recommended in preference to percutaneous coronary intervention (PCI) to improve survival in patients with multivessel coronary artery disease and diabetes mellitus, particularly if a left internal mammary artery graft can be anastomosed to the left anterior descending artery. 9. Coronary CTA should not be performed for assessment of native coronary arteries with known moderate or severe calcification, or with coronary stents <3 mm in diameter in patients with known SIHD who have new or worsening symptoms not consistent with unstable angina, irrespective of ability to exercise.
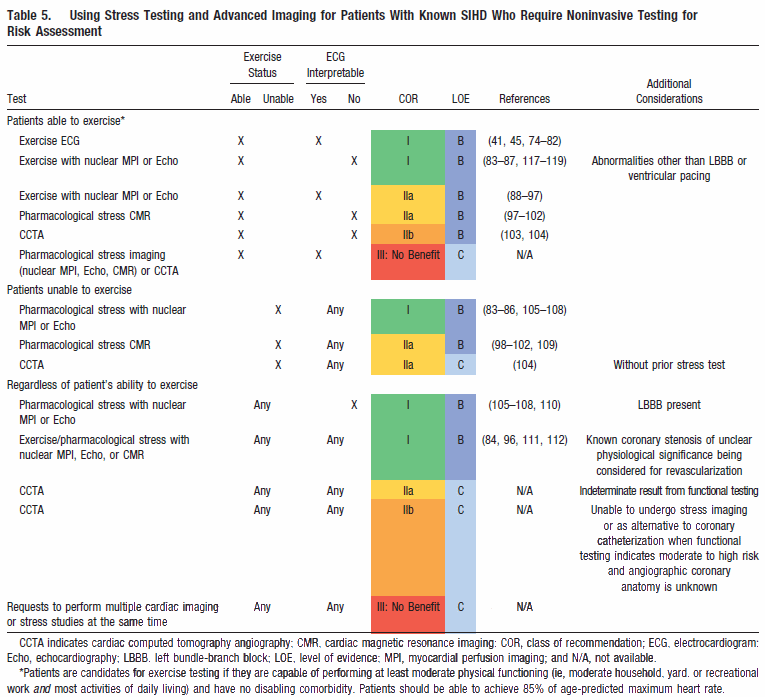
10. Compared to patients receiving
CABG, complete revascularization is accomplished less often in
subjects receiving PCI (e.g., in <70% of patients), and the extent
to which the absence of complete initial revascularization
influences outcomes is less clear. Prashant Vaishnava, M.D., CardioSource, November 2012 |
|
|
|
|
|
*In patients with multivessel disease who also have diabetes mellitus, it is reasonable to choose CABG (with LIMA) over PCI365,380,381,381–386 ( Class IIa; LOE: B). CABG indicates coronary artery bypass graft; CAD, coronary artery disease; COPD, chronic obstructive pulmonary disease; COR, class of recommendation; EF, ejection fraction; LAD, left anterior descending; LIMA, left internal mammary artery; LOE, level of evidence; LV, left ventricular; N/A, not available; PCI, percutaneous coronary intervention; SIHD, stable ischemic heart disease; STEMI, ST-elevation myocardial infarction; STS, Society of Thoracic Surgeons; SYNTAX, Synergy between Percutaneous Coronary Intervention with TAXUS and Cardiac Surgery; TIMI, Thrombolysis In Myocardial Infarction; UA/NSTEMI, unstable angina/non–ST-elevation myocardial infarction; UPLM, unprotected left main disease; and VT, ventricular tachycardia.
|